Featured - The Best Sex Education Articles for Adults
Sexpert.com has the Best Sex Education Articles for Adults from an expert line up of certified sex experts.
Top sex education for adults featured posts and sexuality articles from our sex experts, sex coaches on everything from female orgasms, sexual pleasure, alternative lifestyle topics, couples sex advice and dating advice, masturbation and sexual empowerment, sexual health and wellness including men’s sexual problems like premature ejaculation and how to last longer in the bedroom.
Our Sex Ed featured articles include all the tips and techniques you need to know to make you a better lover such as the ultimate guide to anal sex, BDSM and kinky sex, oral sex, how to have the best orgasms, sexual relationship topics on how to spice up your love life, as well as female sexual anatomy and the erogenous zones including the clitoris, the cervix and cervical orgasm, all about the g spot, female ejaculation and g spot orgasms, the vagina and the vulva, penis facts and more.
Sexpert.com is an all-inclusive sex education site for adults and has many empowering articles on gender and sexuality, as well as articles for gays, lesbians, bisexuals, transgender, sissies, and alternative lifestyles including cuckold and hotwife relationships, threesomes, polyamory and swinging. See our sacred sexuality topics including Tantra sex, yoni yoga, sexy goddess rituals, energy orgasms and more.
Explore sexpert articles from our top sex educators.
Businesswoman Holly Corbella is a first-time nominee for the XBIZ Awards, featured in the category of Retail & distribution – home party company of the year for her amazing company PARTIES BY BELLAS. This fun, vivacious woman has turned Girls’ Nights In into an art–which makes her a prime candidate for a Feminist Sexpert Interviews profile!
FS: What first inspired you to get into the pleasure products industry?
HC: It was not something I ever thought about actually. I wanted to have some fun with my girlfriends so I hosted a girls night in. The party was a huge hit and the lady asked me if I wanted to join so I said sure I’m up for that challenge. It was an amazing 3 years working for passion parties then they unfortunately closed. I was devastated and so was my team. We had 7 days to decide to move over to the company that bought passion parties or cancel our consultant ids. As a team we decided to move over to the new company as we loved The little family we created. It was completely different, so many rules to learn and ways of doing things. Two weeks into the new company I was fired. I hosted a couples party which I was told later on was against the rules. I didn’t know at the time as this was a party I had previously booked. I was told when starting with the new company we had 30 days to complete previously booked partied and transition to the new company. I hosted a mini pity party for myself for about two or three days not being able to leave the house. Then people started to reach out and tell me to start my own business. This was never something I had previously thought of and well the rest is history.
FS: What inspired you to start your own company, and how do you go about it?
HC: My inspiration to start parties by Bellas was my customers, family and fiends. My support system is why parties by Bellas is in Business today. I am truly honored and grateful for all the amazing people in my life. I took my anger and all the sadness I had about losing my business with another company and decided to make a positive spin. I was going to start my own company the way that I wanted it to be!! I was under a one year noncompete so during that time I slowly put together my business. I took online business courses which was some thing that I’ve never done before. I was researching all types of adult products and all sorts of other companies. I just wanted to see what was out there and what was out there and what was missing. From that I started my little family a company that is consultant friendly.
3
FS: The toy domain is one arena of the adult industry in which women hold great power. How do you feel this industry has inspired women?
HC: It feels great as a women to be taking control of my life and my sexuality. I think it takes a strong women to open a business let alone a sex related business. I absolutely love meeting other like minded women and helping them to grow their careers with me. This industry is a great career for women not just because let’s face it Sex is going no where so we never have to worry about that and if covid taught me anything I am an essential worker when everything is shut down lol. Also from my experience unlike any other field I have belonged to these women I have met in the “sex industry” are not ones to tip toe around things they express how they feel. They are having as much fun as I am so the positive vibes surround us. We all help each other to grow and it’s just a great industry to be a part of. We stick together.
FS: How do you feel the party format promotes toy sales? How do you feel that it promotes female bonding?
HC: I feel in-home adult parties is the best way for a woman to find an adult product that is perfect for her. She is able to see the item an how it works before purchasing it. It’s also in a comfortable atmosphere either by herself or surrounded by friends who might have some inside perspective to add to the conversation.Talking about sex is one of the hardest things for people to do. I’ve been told at my parties because I am so open and comfortable about this particular subject it makes partygoers feel comfortable talking about things that they’ve never felt comfortable talking about before. This then brings the women who are at the party together opening up about their most secret of thoughts. Now creating a bond only they will have with each other.
FS: I understand that you’ve been nominated for an XBiz Award? Tell me about it!
HC: Yes, I have been nominated for a XBIZ award! I am beyond excited about this as this will be the first time for me. I was nominated in the category for best in-home parties. I know everyone says that just being nominated is enough and it doesn’t matter if I win. Of course I want to win but this nomination for me made me have my “I made it” moment. I’m up against companies that have been around much longer than parties by Bellas and have many more consultants. Parties By Bellas is still very much seen as a small business as we are just under 30 STRONG.
FS: What are some of your favorite products that you offer, and what are your product categories?
HC: It’s really hard to pick just a few items. I do love our new Bellas kick ass self defense line. I feel it’s very important for a women to be able to feel dave and be able to protect herself. As for the adult line I’d have to say my favorite sex toys are on my website under hollys picks. Just too many to list.
Parties by Bella’s is not just a sex toy company. Yes we have a great selection of sex toys but we have an array of other items such as; self-defense Products, Bath and body items, CBD, Pet products, sexual enhancement items and much more.
FS: How can people learn more about your business? List all relevant websites, social media, etc.
HC: How to connect: I am also a sex life and business coach. I also own an event planning company.
Website: www.partiesbybellas.com
Email: bellasromance@aol.com
Facebook: Holly’s Parties By Bellas
Facebook: Bellas wedding & event planning
Facebook: Bella Lady Boss Life & Business Coaching
IG: Parties By Bellas
Far be it from me, or even you, to determine what it is you are writing until you write it. And even then, you may write a thing, get it all revised, polished and maybe even sell it for a pretty penny, and still come back to change the thing, or later come to morph it into something wholly different than what it originally was.
Don’t keep yourself from this write, revise, morph, repeat process. It can pay you great dividends.
For instance. I scribbled off a very short story once, a first-person narrative, from a mid-40-something lady’s point of view. It was a tale of a sexy (or at least I liked to think it was sexy) flirty happenstance the protagonist made happen that ended up creating more questions for the lady than the answers she originally thought she was going to find. I sold this short. Then, I had occasion to consider the piece anew and revise it as a one-act monologue, which I also sold and sat in the audience watching being ‘put up.’ Since I work across a few different genres and types of writing, I find I can manage this reworking quite often and am pleased when I can. As much because it requires less wholly new writing as it is fun taking a thing that was once one way and seeing if I can make it another.
Now, you surely have to be careful taking something you may have sold or have been commissioned to write, refixing it and then trying to sell it again. Moving forward with something, even a faint copy, depends on the limits of the sale of the work in the first place. A short story and a play are two drastically different animals, but when fixing one story into another, you need tread carefully.
Surely, plenty a short story writer has sold the same story time over and over (again, dependent on the contract particulars of when you sell the story each time) and you certainly can take great ideas from one place or create some characters you might want to see appear in other spots. But mainly I want you to look at your work as having infinite possibilities.
Because, well, it does.
This is why I advise people all the time to just write the thing. Get it out of yourself, down on paper or across the word press document. See it made real, then you can as much figure what it is, what it might still need to become as you can take it and tweak it to be something else entirely or an offshoot of the original thing you made.
Again, the possibilities are limitless when you are open to write, revise, morph and repeat.
If you ever seen an animal program on TV, you have probably seen some of their complicated and interesting mating rituals.
Every animal uses sexual reproduction from ducks to dogs, from lemurs to lemmings, from bats to badgers; even hamsters to humans have mating rituals. These rituals are written right into most animal’s genes and change very little over the millennia.
With humans it’s somewhat different. We have certain prewired responses to all sorts of things, and you’ve probably never even thought about this. For instance, you put your hand on someone’s shoulder to show understanding, concern, and connection. You put your hand on a loved one’s cheek to show closeness and acceptance. And there are many others.
Our meeting rituals are very complex because we are complex emotional beings. We not only use our prewired responses, but we also add in other cultural and social elements. Many of these differ from place to place.
It’s amazing that this knowledge is built right into us from birth. Even babies know how to flirt. In fact, babies are the best flirts around and know right from the womb how to get attention.
You may be asking yourself why do I have to learn how to flirt? Isn’t it built right into me?
Yes, it is, but flirting still takes practice to be an expert at it. As we get older, we need to relearn how to flirt.
After all wide should animals have all the fun??
Why Bother Learning About How to Flirt?
What’s in it for you?
Why should you want to learn these concepts? Certainly, because you want to have a rich, active dating life, but that’s not all. There are many benefits to learning these skills that carry well beyond dating, sex, and relationships.
First of all, flirting is fun! It’s a playful, adult game and lets you interact with others in a safe, playful way. It also builds your self confidence and even gives you new tools to deal with everyone in your life.
Another benefit is that it lets you explore your own “relationship self” by showing it to others. You’ll be surprised at how receptive other people are when you start showing this wonderful part of yourself.
When you are fun, playful, confident, and able to express yourself without shame, embarrassment, or guilt, you can naturally flirt with success.
Find What You Are Looking For
Are you looking for love? Fun? Romance? Sex? Intimacy? Companionship?
All these things start with the same first step. Finding a partner.
Here are some ideas that will help you reach any, or all, of these goals:
Incorporate a situation that in the past proved to be difficult and see that you can handle the same situation with a renewed perspective and acceptance.
Take the plunge and ask out that person you have spin secretly admiring. If your date proposal is rejected, realize that you can survive it. Your target rejected the situation not you. It is far better not to waste time on someone who is unavailable or uninterested. Move on to the next prospect.
Places to meet someone
There are many places to meet new people. In fact, everywhere you go is a new opportunity. Here are a few examples:
Airplanes, at work, auction houses, bars, beaches, bike riding, bookstores, bridge clubs, cafes, at the car wash, while taking classes, dance clubs, day trips, fashion shows, galleries, health clubs, while going for a jog, at libraries, matchmaker clubs, Men’s department stores, movies, museums, music festivals, parks, parties, personal ads, potluck suppers, book readings, restaurants, work seminars, shopping malls, singles events, supermarkets,, theatre groups, through friends, through relatives, at trade show events, on vacation, while going for a walk, and of course, weddings.
How to Flirt
Make eye contact. Don’t stare. Raise your eyebrows. Wink if you’re bold!
A warm sincere smile is like an open door of approval.
Body language. These are the signs people through body language showing you are interested in someone else. These include the hair flip, swinging your leg playfully, the head toss, batting your eyelashes, leaning closer to someone, touching their hand, licking your lips, and cheering them with a toast.
Flirting Prompts
Here are things you can do to get noticed or use as conversation starters.
Carry a book with an eye-catching title.
Where a hat that suits your unique style.
Pin a button on your clothes that has a message to attract attention.
Take your pet for a walk.
Carry a camera and ask someone to take your picture for you.
Apply an outrageous bumper sticker to your car.
Wear clothes with unusual logos.
Drive a unique car or bike.
Conversation Starters
When you open a conversation with someone new, the words you choose to speak can be the most important, especially if you are on a quest to find everlasting love.
Take the seductive approach. This style should stir but not shock.
Try these:
You smell really good. What scent you wearing?
Weren’t you in the Sports Illustrated swimsuit issue?
Didn’t I see you on the cover of GQ magazine?
I hope you don’t mind, but I just had to let you know that you are the sexiest person here.
Do you mind if I sit down? When I saw you, I went weak in the knees.
If good looks were against the law you’d be arrested, booked, and jailed for life!
Can I buy you breakfast in the morning?
I was looking at the dictionary and there wasn’t a word that fully describes your beauty / sex appeal.
Dating Rules
Try these dating rules to become more sexessful at love.
Rule 1. Talk to everyone.
Don’t be embarrassed to let people know you are a single and be proud of it. Let everybody know that you are looking to meet that special someone and, who knows? One of your friends, relatives or acquaintances might match you up with your everlasting love.
Rule 2. You are in control period.
You are in control of whom you decide to date and whether you see that person again. Yet, all single people seem to think the other person holds all the cards. Dating is a wide-open field these days. If two people exchanged business cards or phone numbers, it’s not etched into stone who should call first. Spring a surprise by calling them first. At least you will find out if there is mutual interest. And if you do take the initiative and get turned down, praise yourself for having made the effort to test the waters, then move on.
Rule 3. Dating is not a crapshoot.
You make the choice as to whom you want to date and when. You don’t have to go out with everyone you meet. If you just don’t like someone well enough to date that person, tell that individual upfront you were not interested in a relationship, but you appreciate their interest. Never overlook the possibility of a friendship that may become a romance later on down the road.
Rule 4. Everything is negotiable.
Just because you may want to fall in love with someone who has the same passions as you don’t restrict yourself too much. Remember that everything is negotiable in life and in love.
If you meet someone you like who doesn’t share your lifestyle, be open to learning from each other. Compromises can be reached if you care enough to explore the possibilities. One thing I have learned is that couples can be very creative together when they want to find solutions to the problems that crop up.
Just because you want to fall in love with someone who has a passion for boating, and you meet someone who has a passion for horseback riding, doesn’t mean you can’t spend one weekend on the ocean and the next on the ranch. You can create a win-win situation. Likewise, if he’s a steak and potatoes person, and you’re a vegetarian, be open to exploring and learning from each other. Compromises can always be reached if you care enough to explore the possibilities.
Rule 5. Don’t turn anything down before it is offered.
Don’t read a person on your first meeting. Even if your instincts are right, the relations still could blossom, or you could meet your everlasting love through this person. I cannot stress this rule enough. In the rat race of life, we jump to conclusions about people without even knowing them first. I’ve seen more potentially good relationships bite the dust before they even got off the ground.
Don’t assume you know everything about a person on the first meeting either. Even if you don’t like what you see or hear on that first date, attune yourself to what you do like and see if there is more there. You never know what could happen.
Things to Talk About on a First Date
Below you will find important dating etiquette tips that can often make the difference between making a connection and blowing the opportunity.
Don’t talk about anything negative such as family or health problems.
Don’t talk a boat your financial status and never talk about past relationships especially if they were bad.
Do talk about your goals, work, hobbies, favorite places, and your personal philosophy.
Do ask a lot of questions.
How to Move from Dating to Intimacy
Intimacy is not about wild, rapid, passion. It’s more like an insatiable slow burning passion. Intimacy is about expressing your true feelings not just what you think is sexy to your partner. Touching each other on nonsexual areas is intimate. Intimacy is not about being critical of your partner. Intimacy is not about conquest it is about being present and giving pleasure not just receiving it. Intimacy is about enjoying the journey together.
Intimacy is not just sex, but incorporates trust, comfort, safety, surrender, respect and open communication. The sexiest thing is being focused and present while making love. Both partners must have a clear intention to be fully in the moment rather than being goal orientated. Most people don’t touch each other with intention. It’s a natural evolution that we should find a deeper level of enjoyment, by moving from sex to intimacy.
You don’t have to give up your regular sexual practices. You can add to your sexual repertoire by practising the art of intimacy.
To experience emotional intimacy, you must surrender yourself so that you feel complete to compliment each others souls. You must be willing to let down your defences and open your heart.
Intimacy is the plateau of sex that every couple strives for but must go through all the other steps before they can achieve it successfully. You need to be on the same plane sexually, physically, emotionally, and spiritually.
We ultimately strive for our emotional doorway to open through all of our senses when we are both are present any available, emotionally to one another. You are honoring yourself surrendering and connecting with your soul mate.
Here are Three Steps to Move From Dating to Intimacy:
Step 1. Share your feelings about each other to create an emotional bond.
Step 2. Focus on your partners needs wants and desires and put them before your own.
I don’t think I have to tell you that self care is important to your health and overall well-being? But, just in case you are like me, and feel like you must always be doing something and being productive (like writing this article instead of doing my own self care right now!), and need to be reminded to slow down, take time off and stop neglecting yourself, here it goes:
Stop what you are doing right now and prioritize self-care!
Take a moment to breath that in and visualize what that would feel and look like for you.
Where in your life have you been neglecting yourself? Where do you feel depleted? Feel into your body. Where do you feel tightness, pain, tension, unease, dis-ease?
Take another moment and feel into those spaces of tension, and ask yourself, what would feel good to do right now? Stretch? Get up a take a short walk? Take time to breath deeply? Drink some water? Open the window and let in some fresh air?
Where could you add a bit more self-care into your everyday?
Creating a Daily Self-Care Practice
I like to create a daily self-care practice for myself every morning. This is because it is the time when I will most likely stick to my routine and it also sets the precedent for the rest of the day. But you can take time out any time during the day, even if it for only 5 minutes, and give yourself the rejuvenating nourishment of self care. This is especially important if you sit at a desk all day or have a sedentary life.
Create a Time for Yourself
Below I have added a list of 45 Daily Self Care Tips that you can use, or to help inspire you to create your own. You don’t have to do everything on the list (obs!), but pick just one, or a few that you feel inspired to do each day, as a regular routine. Remember that you can swap out or add on new activities that may be more rejuvenating for you at any time.
Pick a time of day where you will schedule in your sensual self care daily practice “me time” and give yourself 20 minutes (at least) to 1 hour to recharge. You can also schedule in 5-20 minute breaks during the day to add in other self care activities as well throughout your day.
Try this for at least one week and see if you feel a difference.
Believe me, your are worth it, and so is your well-being. Because if you are not going to take care of yourself, who will?
What is Self Care?
Self care is anything you do that makes you feel good and nourishes you. Self-care is the act of engaging in strategies that promote our physical, mental, emotional and spiritual functioning and enhanced well-being.
Prioritizing self-care can help you relax more, manage chronic stress easier, prevent health issues, revitalize you, and make you feel good inside and out.
“When self-care is regularly practiced, the benefits are broad and have even been linked to positive health outcomes such as reduced stress, improved immune system, increased productivity, and higher self-esteem.”–https://www.everydayhealth.com/self-care/
45 Daily Practice Tips
Here are the 45 daily self-care tips you can try. Take baby steps and just add one to start your daily self-care routine today!
Wake up Stretch in Bed
Enjoy breakfast in bed
Brush Your Tongue & Teeth
Gargle with a natural mouthwash (water & essential oils or oil-pulling)
“The Universe contains three things that cannot be destroyed; Being, Awareness and LOVE”– Dr. Deepak Chopra
One situation that makes it difficult to find a silver lining is facing illness. Just consider the
top five medical threats: heart disease, cancer, stroke, chronic respiratory diseases, and
Alzheimer’s disease.
Not exactly a happy list, right?
Illness and Intimacy
Anyone who has suffered from illness knows that feeling of helplessness and fear of a future without intimacy. Maintaining positive mental health can be a tremendous aid in dealing with challenges like this. In fact, while your fears about your partner’s illness may compel you to push away the person you love the most, this could be an opportunity to
enhance intimacy.
Most couples that really love each other discover that their love grows stronger and their passion deeper after trauma because they no longer take each other for granted. They fall back in love and want to treasure every moment. This is the time to start re-creating
romantic memories together, to say and do all the things you did when you first met and some you never did before.
Recapturing Intimacy After Illness
Rabbi Ed Weinberg, Ed.D., DD, offers a lot of great insight into overcoming illness and recapturing your intimacy in his book, Conquer Prostate Cancer: How Medicine, Faith, Love and Sex Can Renew Your Life. Guided by Rabbi Ed’s heart-centered coaching, men and women learn to reignite intimacy physically, emotionally and spiritually — loving and living with renewed joy. He believes that physical intimacy can help a man or woman offset some of their frustrations when one or both have a sexual dysfunction that
prevents intercourse or orgasm.
It’s my pleasure to share Rabbi Ed’s advice on how you and your partner can get your sexual life back despite prostate cancer.
NEURO-CISE: S.T.I.C.K, DUO
1. Decide to “make love,” rather than “have sex.” Physical intimacy can help a man or woman offset some of their frustrations when one or both have a sexual dysfunction that prevents intercourse or orgasm. To offset this, recognize that orgasm is possible for many, although not everyone, even when men can’t have erections due to ED or women have female sexual dysfunctions (FSD).
Don’t insist that your manhood is exclusively based on your capacity for intercourse. Instead of sexual intercourse, make bonding with your partner your main objective. It’s understandable that losing sexual functioning can lead to a sense of emasculation as a man or deficiency as a woman. Still, if you accept that “making love” rather than “having sex” is at the core of your most intimate moments, you may find increasing sexual satisfaction. This is not a question of semantics, but a way to reframe what intimacy is all about.
2. Focus on different body sensations before engaging in intercourse, using the S-T-I-C-K method for “whole body sex.” This is a variation of progressive “sensate focus” for gradually
increasing arousal. Couples may choose to alternate this suggested sequence of sensual activities or combine some of these steps:
S – Stroke each other psychologically. Almost everyone needs to be stroked. Start with verbal expressions of what you admire most about each other and what attracts you to each other intellectually, spiritually, emotionally, and physically.
T – Touch each other physically, starting with a hug, whether clothed or not. Proceed to mutual massages, front and back, gradually progressing from your shoulders to your waist,
avoiding your partner’s breasts. Then proceed to touch or massage each other’s legs before gently caressing erogenous zones like each other’s breasts, thighs and genitals.
I – Intercourse can be attempted right after stroking and touching, or later if you are “up” for it – but don’t rush it! Many men, including early stage and advanced prostate or breast
cancer patients and survivors, may find their sexual frustration persists despite the satisfaction they can derive from whole body alternative sex play. If ED or FSD persists, the couple can consider a soft entry approach, with the man’s flaccid penis rubbing the surface of his partner’s genitalia. Using a dildo and harness can also be mutually satisfying, and if both partners apply lubrication both men and women can make this a more pleasant and pleasurable experience. A penile implant, requiring about 1 1⁄2 hours of surgery, is another option for men to eliminate ED altogether.
C – Cuddle without initial expectations of anything but deriving warmth and support, physically and emotionally.
K – Kiss each other gently on the lips, cheeks, and back. Then go below the neck, but above the waist. From there, your lips can go elsewhere, if mutually acceptable (compare “T”). Adding a mixture of whipped cream or your favorite chocolate can heighten your pleasure.
3. Communicate openly and often with your spouse or partner. Be truly present when talking with your beloved about non-sexual matters. After all, you can have smooth, ongoing relations only if you have a good relationship! Set aside time to talk with your spouse or partner about your personal needs, especially sexual intimacy. If talking explicitly about sex is awkward for either of you, you can each write down what you need or want from each other and then compare notes and follow up.
Explore alternatives as well like tantric sex exercises, originally derived from 6,000 year-old Indian practices that help lovers focus on each other for a prolonged time. This involves mutual eye contact and parallel movement and breathing, to become fully present and
at one with each other and potentially multi-orgasmic. Attending a Marriage Enrichment weekend retreat can also reinforce your connection with your significant other on many levels.
4. Schedule times to rev up your romance. Sexual relations are hard to sustain without developing a good relationship. Set dates with each other to allow for greater nonsexual intimacy, such as seeing a movie or going to a restaurant or concert together. Use scented candles and wear special pajamas or lingerie (or nothing at all!) with soft lighting, to set the mood for increased physical intimacy.
5. Watch a hot movie together that appeals to your sense of humor. Agree to rent a steamy film for home or hotel room viewing to help get you and your partner in the mood to become physical. Make sure you do not choose a film that is going to turn one of you on, but the other off, and remember that a humorous show can warm you up to each other! Keep in mind that some educational films, though approved by sexologists, may be boring and fail to arouse couples, so preview films to see what works best for you.
6. Develop a healthy lifestyle. Exercise regularly and eat a balanced, heart-healthy, low-sugar diet for weight control and improved sleep. Reduce alcohol intake to avoid sluggishness and eliminate smoking to enhance genital blood flow. Such steps can renew your level of energy and reduce performance anxiety. Let your mantra be, “I enjoy my sexercises” to maintain penile or vaginal blood flow through self or mutual-stimulation. Start this as soon as possible after a health procedure such as cancer surgery or other procedures, in consultation with your doctor.
Daily Kegel exercises, with the help of biofeedback if needed, can strengthen your pelvic floor and sphincter muscles. While these won’t raise your libido, Kegels can help with ED and FSD. They will also help “stem the tide” for those with mild incontinence.
7. Keep the faith. To conquer ED or FSD and raise your libido, have faith in your Higher Power, your doctor, your spouse, and above all, yourself. Regarding sexual activity as sacred or purposeful can make for a more powerful experience.
It’s important to recognize that stress, treatment side effects, and the aging process can affect not only seniors but boomers and younger men and women as well. Simply knowing you are not alone in your efforts to renew your life physically, emotionally and spiritually can help. It’s equally important, though, to realize that you can bounce back from ED/FSD and a low libido if you resolve to rely on your resilience and your adaptability to new forms of sexual expression.
This kind of faith can raise you to new heights!
Breast Cancer
With over 280,000 new cases of breast cancer each year in the United States, there are over 2.5 million survivors of breast cancer. According to the National Cancer Institute, about one out of every two women who have undergone breast cancer treatment experiences some kind of sexual dysfunction.
When a woman has a mastectomy to remove all or part of her breast(s), her body may be capable of sexual response, but sexual desire is one of the last things on her mind. It’s no surprise that many women feel very distressed after a mastectomy as in our culture breasts are viewed as part of a woman’s femininity and sex appeal. Not to mention that touching breasts is a common part of foreplay and she will no longer want or be able to experience the same way as before the surgery. Breast reconstruction may restore the shape and size of the breast(s) and help a woman to feel more attractive so that she can enjoy dating or being sexual with her partner, but the physical and emotional healing process is much bigger than a simple cosmetic fix and requires a tremendous amount of time, understanding and respect.
Being single and dating when diagnosed with breast cancer is even more challenging as talking about it to a potential romantic partner can be very awkward and scary. Nevertheless, getting out and socializing is part of the healing process and will help you to
feel normal again. There is a fine balance that needs to be walked between respecting your own needs while also trying to push yourself a bit beyond your comfort level in order to reengage with the world.
Small steps are important because even the smallest connection with another person can aid the healing process.
According to the American Breast Cancer Society, breast cancer is about 100 times less common among men than women. For men, the lifetime risk of getting breast cancer is about 1 in 1,000 compared to women at about 1 in 8. Twelve percent of women in the U.S. will develop invasive breast cancer during their lifetime.
Undergoing extensive treatment from surgery to medication, chemotherapy or radiation can be detrimental to your sexiness. Stress, anxiety, changes in body image, side effects of treatment, pain, hormone fluctuations and depression can negatively affect your libido. However, the good news is that you can heal and regain your sexual health.
Spinal Cord Injury
Research by Barry Komisaruk, Beverly Whipple (“The Science of Orgasm”) and their colleagues has shown that women with complete spinal cord injury can respond to vaginal or cervical self-stimulation because they could perceive it, with some reporting an orgasmic response. A spinal cord injury, traumatic brain injury, or major illness does not diminish a person’s sexuality, although it may change a person’s feeling about sex.
Intimate communication with your partner can be challenging, but remember nobody can read your mind, so tell each other what is working and what isn’t. Being direct with other people helps the relationship grow. However, some people who have intellectual or physical disabilities may find it hard to express their anxieties about body image or limited sexual function. Show your personality and humor during these uncomfortable moments because laughter can make the situation more comfortable.
Thinking Off
If there is an inability to experience sexual release, some say that sexual energy can be moved up into the mind. Channel, build, utilize and move the energy into having a mental orgasm. Start by visualizing the orgasmic flow inside you, knowing that orgasm is within and focus on erotic feelings that lead to physical tingling orgasmic waves as they pulse through your body.
There has been some scientific research on energy orgasms. Most notably, Dr. Beverly Whipple calls it “Thinking Off ” and says that you can use imagery alone to reach an orgasm, but the idea of thinking yourself to orgasm is not new. In the early 1970’s, the Masters and Johnson research team documented the strong connection between sexuality and thought. The connection is particularly strong in women, says
Dr. Ian Kerner, “The brain is the most powerful sex organ.”
Robert Palmer - Addicted To Love (Official Music Video)
Might as Well Face You’re Addicted To Love
“My fear of abandonment is exceeded only by my terror of intimacy.”– Ethlie Ann Vare
“Addicted to Love” was a hit song for Robert Palmer in 1985 and remains a perennial pop favorite today, but the reality of love addiction isn’t so much fun.
Being in love feels fantastic but not when it crosses into obsessive thinking, manipulation, crippling fear, and panic attacks. If self-worth and happiness all hinge on a romantic relationship, it places a stranglehold on a healthy life. This overwhelming need, this
starvation for love, thrives on a dangerous blend of high expectations and low self-esteem. The ‘love addict’ begs for a love that he or she feels unworthy of, creating a no-win situation.
In her book, Love Addict: Sex, Romance, and Other Dangerous Drugs, Ethlie Ann Vare offers incredible insight into the rarely discussed affliction of love addiction. By using alcoholism as a comparison, she found that many of the psychological and behavioral issues were the same, which indicates that, like the difference between a heavy drinker and an alcoholic, there is a difference between someone who loves love and a love addict.
There really isn’t a strict test to decipher if you’re a love addict, but Ethlie offers a series of statements to consider that may indicate a problem.
Here are 10 of them:
1. I often feel an instant connection to someone I’ve just met.
2. I consistently choose partners who are emotionally, geographically, or logistically unavailable.
3. I have passed over family, social or career opportunities in favor of romantic and sexual ones.
4. I use sex to hook a prospective romantic partner.
5. I have considered, threatened or attempted suicide over a relationship.
6. I feel worthless when I am not in a relationship and jump into the next one as quickly as possible.
7. When I’m attracted to someone, I often ignore warning signs that this person isn’t good for me.
8. I am possessive and jealous when I’m in love.
9. I like to be the pursuer in the game of love, even chasing after people who have rejected me.
10.I have been dependent on drugs, alcohol, gambling, spending or food in the past, but most people think I have my life together.
Again, this is not a scientific test and it’s actually possible to answer “yes” to all of them
and not be addicted to love. However, your gut reaction to the questions and the intensity
with which you can answer “yes” is a good indication of whether or not you should take a closer look. The concept of love addiction is incredibly complicated, largely because it is so hard to understand. As Ethlie puts it, “Sex and love aren’t the problem. They are someone’s solution to a problem we don’t understand.”
Photo by Engin Akyurt from Pexels
As described by doctors Harvey Milkman and Stanley Sunderwirth in their book, Craving for Ecstasy: The Consciousness and Chemistry of Escape, the brain’s reward system has three divisions:
1. Arousal: gambling, cocaine, extreme sports, sex
Romantic relationship elements are the only ones that cross all three divisions, making love addiction quite intense. What helps define behavior as an addiction is the obsessive element. A desire for love is replaced with an obsessive need for love that can lead to stalking tendencies, excessive relationship “hoping,” and mistaking every “hello” as an invitation for romance.
The brain chemicals most associated with love addiction are dopamine, serotonin, vasopressin, oxytocin, and phenyl- ethylamine (PEA), with others like testosterone and adrenaline coming into the mix as well. While all of these elements play a big part in a healthy romantic relationship, it is the miscommunication between these elements within the addict’s brain that causes problems. In Healing the Addicted Brain, Dr. Harold Urschel uses the analogy of a phone call to describe how this miscommunication happens:
If one cell is trying to speak to another cell but doesn’t have enough of the necessary neurotransmitters, it can only whisper its message or even become mute. If it has too much of certain neurotransmitters, it may send an incorrect message. Conversely, if a cell is trying to listen to another cell but doesn’t have the proper assistance, it will only hear the message faintly, if at all. Or, if the cell has too many of a certain receptor, it will ignore the messages of others. It’s not an imbalance that happens as much as the addict brain isn’t using what it has properly. The trigger, whether it is cocaine or a new relationship, gives a short-term boost to these transmitters, causing a chain reaction through the brain’s reward center, which in turn creates a hunger for these euphoric feelings.
Love addicts can feel a gaping hole in the center of their lives when they are not in a relationship. It is in his or her nature to quickly, desperately find the next partner, simply to have someone, anyone, to give their life meaning. It is easy to focus on the potential of
something instead of the reality of it. You must look at your situation as an outsider and examine the facts as they are today.
Is this relationship healthy?
Are my needs being met?
Have I accidentally placed my partner on a pedestal?
Are we equals or am I the only one willing to compromise?
Sadly, making the choice to stop loving in an unhealthy way may result in the need to end a damaging relationship. A partner, who has been treated like royalty, with no need for compromise or equality, may not know how to give you the healthy relationship you need.
Even the end of a bad relationship needs a grieving process. It helps cleanse the psyche so the same negative patterns don’t get repeated. Give yourself time to fully feel the loss and try to find the positive things that you can take away from the experience.
Addicted To Sex
Photo by Nathan Cowley from Pexels
Enjoying sex certainly isn’t a cause for concern, nor is a desire to have sex often. However, there is a line that can be crossed when desire becomes an obsession and that’s when things become troublesome and dangerous.
Sex addiction afflicts someone that has a compulsive sexual disorder with no (or little) self-control. It is believed that as many as 30 million people in the United States suffer from some level of sexual addiction.
Consider the following questions that are used to define someone’s level of addiction:
1. Do you think about sex so often that it interferes with your concentration?
2. Are you obsessed with a specific person or sexual act even though it brings you cravings and discomfort?
3. Are you finding your sexual pursuits affect your ability to manage your life?
4. Do you HAVE to flirt?
5. Do you feel you are entitled to sex?
6. Would life have no meaning without sex?
7. Do you think that sex is the only thing that really gives you value?
8. Do you use sex as an escape from other problems or stress?
9. Do you keep a list of the partners you have been with?
10.Do you need the “high” that the dangerous sex and the risk of being caught can promise?
If your answer to all these questions is “yes”, then you possibly suffer from sexual compulsion. Sexual addiction is a relatively new addition to psychosexual disorders. People were simply defined as being hyper-sexual, players, promiscuous, and not wired for
monogamy.
“Sexual addicts are willing to sacrifice what they cherish most in order to preserve and continue their unhealthy behavior.”– Dr. Patrick Carnes
It was as recent as 1983 that sexual addiction first came to the front and center of the news as a legitimate medical concern upon the publication of Out of the Shadows: Understanding Sexual Addiction by Dr. Patrick Carnes. These hyper-sexual behaviors are
oftentimes connected to other addictive or obsessive personality traits, psychological disorders, self-esteem issues, self-destructive behavior, hereditary addiction issues, and lowered sexual inhibitions.
A sexual addict’s mind is sparked the same way as most addictions occur. The brain tells
the sex addict that having illicit sex is good the same way it tells over-eaters that over eating is good. The addicted brain fools the body by producing intense biochemical rewards (levels of PEA phenylethylamine) that boost euphoria for self-destructive behavior.
There are three-stage progressions in becoming addicted:
1. In the first stage, the person actually believes that his or her addiction is healthy, normal, and pleasurable.
2. In the second stage, the person has conflicting thoughts about whether or not the addiction is healthy, normal, and pleasurable.
3. In the third stage, the person realizes that they are addicted and feels unhealthy, abnormal, and more pain than pleasure, yet he or she maintains and feeds the addiction.
The key is to discover the thought processes that are at the base of the addictive behavior and working to replace them with healthy behavior or eradicate them. Trauma, grief, previous abuse, anxiety and depression have all been linked to sexual addiction. In these
cases, the act of intercourse is not treated as something sexual, it becomes medicinal. The endorphins, serotonin and testosterone of sexual activity and release create the bandage that briefly soothes the deeper, untreated pain.
The four most common methods for treating sexual addiction are the same as treatments for any other addictions:
1. The Twelve Step Programs
2. Psychotherapy
3. Sex Addiction Treatment Facilities
4. Spiritual Intervention
Like food addictions, sexual addiction can be challenging to treat because sex is an important part of life. It’s our second basic instinct after survival, and unlike learning to function without drugs, alcohol or cigarettes, learning to function without any sex at all is not possible when trying to build or maintain an intimate relationship.
Photo by Anastasia Shuraeva from Pexels
Understanding how a healthy sexual and intimate relationship looks and feels can be difficult after sexual addiction treatment. As a child abuse survivor, recovered sex addict, and therapist, Maureen Canning speaks from experience as she identifies the 10 characteristics of a healthy relationship in her book Lust, Anger, Love: Understanding
Sexual Addiction and the Road to Healthy Intimacy.
1. Sex provides a feeling of wellbeing.
There is a safety in a healthy relationship that may be a bit scary at first. It will take patience and perseverance to move beyond the feelings of disconnection and shame that may have been part of the previous sexual experiences.
2. Emotional and physical sensations are more positive.
Romantic intimacy requires vulnerability and emotional honesty without numbing or “chasing the orgasm.”
3. Creativity and passion are rediscovered.
As sex is no longer the only outlet for emotional expression, the brain learns to use these tools for creative exploration in new ways.
4. You nurture yourself in non-genital ways.
Pleasure is expanded beyond the previously exclusive channel of sexuality to include all aspects of life.
5. Suffering is tolerated as a part of life.
When life’s challenges, disappointments, and difficulties come along, they are dealt with in a more cerebral rather than sexual way. They are faced, not hidden.
6. You can be emotionally vulnerable.
It is common for sexual addicts to fear betrayal and to suppress their feelings instead of risk being hurt. In a healthy relationship, vulnerability is not only acceptable but also necessary.
7. You develop and maintain healthy boundaries with others.
Boundaries are the enemy for many addicts and in some cases work as the trigger for destructive behavior. Acknowledging, accepting and embracing the safety within these romantic boundaries are an important part of recovery.
8. Sexuality is well balanced and moderate.
Sexual energy in all its extremes is used to motivate the life of a sex addict. With sexual maturity comes the appropriate flow of this energy.
9. You are curious and caring about other people’s reactions to you.
Whereas sex addiction is very ego-driven and the emotional lives of others are kept at a distance, healthy intimacy requires empathy and understanding for your partner’s point of view.
10. You learn to trust others.
The first step in overcoming sexual addiction is learning to trust yourself and accepting the truth of who you are. This personal trust gives you the courage to lower your guard
enough to invite in the truth and trust of a partner.
If you or a loved one is experiencing sex addiction, these resources may be helpful:
Nov. 7 would have marked the birthday of Dirk Shafer–a man who, sadly, did not live to see it. The director, model, writer and fitness expert passed away in 2015.
I never knew Dirk–but when Young Feminist Sexpert was in college and a devoted reader of Playgirl magazine, he counted among my top crushes. Dirk was Man of the Year!
A George Michael lookalike who also wrote for the magazine, Dirk seemed in many ways to be a like-minded soul–one who, like myself, had an interest in writing, movies, acting, and, well, sex. Duh! Among my favorite Dirk-stinctions was the striptease that was photographed step by step for the pages of Playgirl, and his declaration that he liked to work the PG phone sex line because he loved to relieve the stress of a woman’s day through verbal and visual stimulation–to get somebody off on a hot, steamy night. Aye, carumba! He also wrote witty articles for Playgirl, talking about his ongoing campaign to promote ERH (Equal Rights for Hunks), and relating a touching story of meeting a fan who–while not conventionally beautiful–dazzled him with her kindness and humor.
And, yeah see, that was really why I liked him. His wit and sensitivity. The flawless abs, penetrating eyes and captivating–um–smile were just a big collective extra. Really. I mean it.
As Man of the Year, Dirk had announced his intention to make a movie about his Playgirl experience. Thrilled at the prospect, I told myself I’d be the first in line to witness this sure to be amazing cinematic opus. And a year or so later, as a newly graduated journalist at a small-town newspaper, I was enjoying a lazy Saturday morning in the bathtub when I heard a news bulletin incoming from a TV in the other room–announced as such on the most credible and relevant news channel that a fledging journalist could watch. E! Entertainment News, of course.
“A former Playgirl Man of the Year has made a movie about his experiences,” he said. “And in the film, he made a startling announcement.”
“He’s gay.”
Um…wut? Surely I got some water and Pantene pooled up in my ears. I did not hear that correctly.
Ah, but it was true. Dirk’s big movie, Man of the Year, concerned the fact that he was indeed homosexual.
No worries. I didn’t try to drown myself in the tub. But I did feel a mixture of emotions that was difficult to describe. A little proud of Dirk for making his dream film, and being open about who he really was. A little sad that he didn’t like girls. A little deceived.
Deceived, not because I have anything against gay people–but because this man had presented himself as a woman’s fantasy lover, and even gave advice on talk shows about what women want. He apparently asked his best female friend to pose as his girlfriend, and his boyfriend to pose as his roommate. He went so far as to agree to a fantasy ‘dream date’ with a magazine contest winner, all the while trying to dump her so he could retreat to his hotel room and be with his boyfriend. Apparently she caught his bf hiding in the shower. Look up the word ‘awkward’ in the dictionary, you’ll probably spot a screen cap of this very scene.
I reflected on my college years, and how–as a sensitive and starstruck 19-year-old–I believed literally everything I read in Playgirl. I read one centerfold interview in which a gorgeous blond said he was single and looking for Ms. Right–when I looked back at his layout a few years later, I noticed for the first time the wedding ring that shone brightly from his hand. Eventually, I saw him and his wife being interviewed on a talk show. He’d already found Ms. Right, and she was the one who’d submitted his photos for consideration to Playgirl. So I guess that, upon initial inspection of his layout, I had been too busy perusing other parts of his anatomy to pay overmuch heed to his darned ring finger.
I also recalled the fact that, while taking a magazine journalism class, I had created a dummy magazine called Real Woman; an anti-fashion magazine devoted to the average, hardworking women of this country. I included a fake article about a male model who preferred ‘real’ women over female models, and illustrated the article with Dirk’s photos.
Well, guess I was half right. He didn’t date female models.
In the months that followed, I shared my feelings with several friends–all of whom had varying reactions. One was out and out ticked, saying that Dirk should have been open about his sexuality from the beginning, thus performing a real service for gay people through his openess, and for women by presenting himself as someone who could be their best friend–someone who wouldn’t objectify them. Others shrugged and said, “He did his job. He provided a fantasy, and–during the time that he was Man of the Year–he gave you something to dream on.”
When Man of the Year was released, I was en route to a Florida vacation with my parents. We stopped at an IHOP before making the next leg of the trip, which would take us through the beautiful city of Atlanta, Ga.
In looking over an issue of the Atlanta Journal-Constitution as I ate, I saw an ad to promote the film. Suddenly my being was flooded by that same odd mishmash of feelings. I still didn’t quite know what to think of all this.
Just then I heard my mother, aka my best friend and the center of my universe, making some odd cooing and gurgling sounds. Concerned that a morsel of pancake had gone sideways down her windpipe, I raised my head to investigate; only to find that she had met an adorable sister diner who was all of about a year old. I joined her in gushing over and admiring this magnificent little human being, sharing a sweet moment with her and both of our mothers.
Then I finished my meal and joined my parents as we drove through downtown Atlanta in the predawn hours–and you know, if you haven’t seen Atlanta all lit up at night like a Christmas tree, the Feminist Sexpert recommends it.
It was then that I had an epiphany of sorts; a revelation that had to do with cherishing the little moments in life, letting go of the past and embracing the joy that you feel here and now, in this moment.
Years later, after relocating to Florida, I was working as a librarian’s assistant (take just a moment to picture The Feminist Sexpert as a librarian. Scary, I know) at a Tampa library when I spotted a schoolbook that featured a cover photo of a very handsome model dressed as a policeman.
Yep, it was Dirk; a man who could boast cover shoots with both Playgirl Magazine and The Kids’ Career Guide. Let’s hear it for career diversity.
I myself ended up working for Playgirl a few years later, as a fan club president, marketing writer and columnist. At that time, both of the stunning Men of the Year that I helped promote, Charles Dera and Niko, went on to be major stars of straight porn.
Yet if I had encountered a gay centerfold, I like to think that I would have treated him with respect and caring.
Dirk Shafer was 52 when he passed–he himself should have had many more special moments in his life. An inscription on his Hollywood grave reads, “Our Man of the Year.”
Upon hearing the news of his passing, I recalled yet another moment from college; the moment that I ventured in to my campus bookstore to buy his Man of the Year issue.
“I’m so reading this for the articles,” I informed the young lady at the checkout, who replied with a grin, “Now don’t hand me that.”
Suddenly every female in the place, be they shopper or employee, surrounded the counter; with one of them pointing to the magazine cover and asking, “Who is that?”
If you are a past reader of this column, you will have learned that I make my daily bread scribbling my naughty little fictions, reviewing adult toys, blogging for porn sites, as much as I do ghostwriting for various clients. In this regard, I have penned books by dentists, insurance how-to’s, and quite a few memoirs, all anonymously, letting the person I interview for the book, and the person paying me to write it, stamp their name on the tome. It’s been fascinating work, has made me some great client/friends, and takes me far and away from having to write about the latest male masturbator making the market or ruminating over some latex outfit Cardi B happened to wear in her last video.
But as you can rightly assume from the word ‘ghost’ in ghostwriting, nobody knows I have written these books. In fact, I just landed a job at a very big adult business portal, maybe the biggest adult business portal, (a sure fact I am sure proud of) but most of the work I will write here will be anonymous too. I will be given no byline. Nobody but a select few will even know which pieces I write, unless I report on them… which I have been told I can do. But generally, once again I step forward in my career, and believe me, working for this place IS a big step forward, without my name attached to my work.
How does this make me feel?
Give me the work, I say. Maybe if I was younger (lots younger than I am now, I am very crusty and old) I’d care to make noise, rubber stamp my name and likeness across everything of mine that’s out there. Maybe I wouldn’t even take ghostwriting assignments, feeling that all I produce should have my name on it, at the very least. But I lead a quieter existence these days. You won’t much find my picture at too many places (yes, it is at the bottom of this column, but generally very few places) and I’d much rather fade into the background in what I do.
I think writers, generally, are of this mind set. Sure, we all like a pat on the back, some reading groupie coming up at a book signing, stripping down their pants and asking us to sign their thong (men and women both). But generally, scribbling for a living is a solitary endeavour. We do it because we like to be quiet, be by ourselves.
Plus, I am not so vain, well at least not so vain anymore, that I would let my ego get in the way of a job. Sure, I used to be all about the bluster, the ballyhoo, but this was in my younger days when what I produced, be it music or words, was not of such high quality as I produce now… if it is of any quality at all. I think I all but “blew my load,” being so brazen, shaking my ass on stage, literally, and wanting to be seen and heard as much as I was. Again, I was much younger. But youth, they say, is wasted on the young.
Believe me, the last thing you’d want to see is me in a pair of leather pants these days!
You have to come to your own comfort level with all of this. As much as the salary you will demand for your work as what else you want along with it. In fact (and this stays just between us, ok?) that new position I just acquired is not paying me anywhere near what I usually get for similar writing jobs. But I want ‘in’ with this company, I know the work will be fun and easy. And mostly, something steady, which this job seems to be, even a part time regular gig, is manna from heaven for a freelancer. That my name won’t go on the pieces is not a deal breaker in this instance.
Now here’s a little tidbit on that ancient ritual we all look forward to every year; The New Year’s Resolutions. Did you know that it started in 153 B.C. when the Romans named the first month of the year after Janus, the dual-faced God of Beginnings? He is the symbol for resolutions because he could look backward and forward at the same time.
Always make your New Years Resolutions positive action steps for change. Plan, prioritize and then reward yourself when you have accomplished them.
I’d like to share three of my personal New Year’s Resolutions with you.
1. Learn Something New
I must admit that I’m addicted to knowledge and am always ready to learn something new that I can then share with others. Some of the most exciting things I’ve learned include painting, pole dancing, ballet, meditation, Shotokan karate, Tantra and BDSM. The emotional feelings that I get from learning something new includes a sense of accomplishment, satisfaction and confidence. What would you like to learn in 2022?
2. Help Others
The emotional feelings that you can get from helping others includes happiness, greater value and appreciation, inspiration and motivation, and a sense of purpose by bringing joy to others. Whether it’s helping a friend by simply listening to their problems or giving a stranger a compliment to help them feel good about themselves, you can impact someone’s life in helpful ways. So make a list of ways that you can help others.
3. Balance My Life
Plan to bring greater enjoyment into your life by making appointments for more fun, romance, travel and even relaxation. Give up activities that drain your energy or make you feel unhappy. In fact, I’ve come up with my own criteria to say, “Yes” to offers. For business, my criteria are that it must be fulfilling, rewarding, worthwhile, profitable or highly visible. For my personal criteria, the activity must be inspiring, relaxing, unhurried, harmonious, or fun. How will you balance your life?
Now, list your own resolutions. To fulfill your objectives, visualize the end result of each one and tap into the emotional feelings that you will get from accomplishing them. Turn your New Year’s Resolutions into life-changing goals.
Here are 10 Relationship Resolutions
Set a Romance Goal – Hold hands, kiss daily, make time for make-out sessions at least 3 times a week and take turns initiation romantic dates such as candlelight dinners or movie night.
Set an Intimacy Goal – Listen to each other, be emotionally supportive, share your feelings and make love with eyes open at least 2 times a week.
Set a Communication Goal –Ask your partner how you can be a better spouse or lover. Praise your partner often, give him or her a compliment every day, listen more, argue less, verbalize appreciation more and criticize less.
Set a Collaboration Goal – Spend quality time together by doing things you both enjoy. Learn a new hobby together, take dance classes, Loveology online classes, cooking, yoga, camping, painting or volunteering for a charity.
Set a Habit Changing Goal – Make a pact to help each other lose weight, stop smoking, procrastinating, being messy, lazy, grumpy or any other bad habit where you can support each other to quit.
Set a Fun Goal – Play indoor and outdoor games like you did when you were a kid. From hide and seek to pillow fighting, be silly and playful to put the fun back into your relationship.
Set an Intention Goal – Write a couples mission statement and include where you see your relationship in one year. Then frame it in your home as a personal and public reminder of your shared relationship mission.
Set an Improvement Goal – Change something about yourself to make your relationship even better. For example, make an effort to dress up and greet your partner with a kiss after work, learn how to give a sensual massage or just get a fashion makeover.
Set a Forgiveness Goal – Let go of past hurts, open up your heart and let love in with a fresh New Year’s start. Write a forgiveness letter to yourself or to someone who has hurt you, but end the letter by writing that you forgive.
Set a Happiness Goal – Know what makes you happy individually and as a couple. Then live your life to the fullest by doing the things that make you happy, whether it’s eating ice cream, being pampered at a spa or cuddling with your partner.
Be realistic when setting your New Year’s Relationship Resolutions. The reality is that a consistently successful relationship takes compromise and commitment.
Sexy Positions
You can tell a lot about someone’s personality from the sex position they like best. If classic Missionary is your go-to, then you may be romantic, but not very adventurous, or if Sideways is your favorite, you may be the cuddly, cozy type. But whatever your preference, the New Year gives you a reason to expand your repertoire, try something new and think outside the sex box!
1. Missionary
What can we do for Mr. Missionary who needs to spice things up? How about flipping the woman on top? You’ll still have plenty of thrust capability, but this gives her a chance to take control of her pleasure by grinding her pelvis as hard as she wants for G-spot stimulation. Located about a third of the way between the vaginal opening and the cervix, this spot can be stimulated by the penis, especially when the guy lays back. He can easily bring her to orgasm in this position with added stimulation to her clitoris. By the way, men who favor the ‘female superior’ positions are voyeurs eager to please their lovers.
2. Sideways
Sideways positions are great for slow gentle rocking motions and sensual intimacy. For example, spooning is comfortable for the heavy-set or pregnant, and face-to-face scissors position allows easy access to kissing and caressing. But since deep penetration is hard to accomplish this way, a sideways junkie can switch things up by lifting the woman on top of his penis so she can rock her hips from side to side for a different type of sensation, stimulating one of her hidden treasures known as the U-spot, which is the opening of the urethra located above the vaginal opening and outer lips at either side of her vagina.
3. Doggy Style
Doggy style lovers are goal-oriented and the horniest of all the sexual personalities, so don’t blame them for being rough and ready at any time in any place. After all, they are alpha dogs by nature! Let’s look at some doggy variations worthy of a New Year’s Resolution. Try Standing Doggy, which takes more strength, balance and coordination, and is always a memorable choice. I would encourage starting with Vertical Missionary position standing against a wall or a door. It’s great for eye contact and kissing, and then when the intimate passion is amped up, turn the woman to face away for a more animalistic standing rear entry position. For a further variation, crouch down like a tiger and press your body against hers as you enter her from a deep and intense angle that is sure to stimulate her A-spot. Nicknamed for the ‘Anterior Fornix,’ this spot is also known as the ‘Female Prostate’ and is located beyond the G-spot. If you’ve already found the G-spot, then locating the A-spot should be a piece of cake. It’s deep inside the vagina on the upper (anterior) wall where there is a narrowing of the cervix of the uterus that feels like a circular indentation. Putting some gentle pressure on this ‘Frisbee around the cervix’ area can produce rapid vaginal lubrication and intense orgasms, even in women who are not naturally responsive sexually.
4. The Boar
Another orgasmic position is one from the ancient Kama Sutra known as Varaha (The Boar). Like the doggy, this position begins with the man penetrating his lover from behind, while the woman rests her forearms on the bed or floor. This props her rear end higher than her head and opens her wide, putting him in the direct path toward her G and A-spots. He can slide one or both hands up to her shoulders for leverage as he thrusts deeply and she can stimulate her clitoris to supercharge her pleasure. If The Boar becomes your favorite sex position, you are anything but a bore, as both the giver and receiver’s sex personality is wild and animalistic in nature, complete with the grunting and growling of pure lustful freedom. For more exciting Kama Sutra positions, check out my latest book The Idiots Guide to Kama Sutra, with full-color photos and descriptions of extra ways that you can find the most satisfying positions.
With the New Year upon us, now’s your chance to impress your lover and find deeper satisfaction through new sexual positions. By stimulating different muscles and triggering intense emotions, you can make sex feel even better and last longer. Communication is key to find out which positions please you and your lover the most. Sometimes a position you’ve never liked before can become a new favorite with the right variation.
May all your wishes come true for a passionate, prosperous and pleasurable New Year!
Anne Rice died on December 11th, at the age of 80. Known chiefly or at least initially, from her “Vampire Chronicles” (starting with the publication of Interview with the Vampire, in 1976), the lady went on to write over 30 books, straddling many genres.
For me, and as should come as no surprise, considering this column you are reading, it was Rice’s erotica that touched me most.
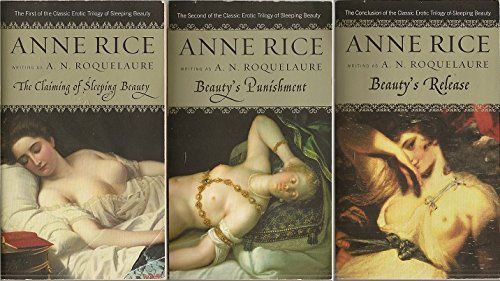
The lady’s BDSM takes on the Sleeping Beauty myth in her “Beauty” series, her Exit To Eden (I warn you, never ever watch the movie made of this book!) as well as my favorite Anne Rice, and one of my favorite books of all time, Belinda, all pack a naughty spellbinding punch and brought me to the realization that not only could Rice write (which I knew from reading plenty of her other books) but she was a world-class erotica scribe.
And there was a fair amount of drama that spoke to me personally, in Anne Rice’s journey and in how she exposed her writing in the sexy genre.
In 1985 I bought the aforementioned Exit To Eden from my local mall bookstore (man, how I miss those bookstores, and just hanging out at the mall in general). I had no idea who the author of that book, Anne Rambling, was, but lifting the hardcover down and giving it a quick perusal, I realized here was a hot little tale, well-written and unlike anything I had come across lately. I devoured the book and turned on a handful of my friends of like-minded sensibility to it.
They couldn’t put the book down long enough to touch themselves adequately, most admitted.
Fast forward a year later, the hardcover Belinda hits the shelves, and I am shocked, yet thrilled to see, printed on this book’s lurid cover (which has turned away too many readers, I am sure) that the author of Belinda was “Anne Rice writing as Anne Rambling.” Rice would also pen her “Beauty” books under a pseudonym, A. N. Roquelaure. Pretty much pouring out books of all stripes, and even though investing her vampire fiction with a goodly amount of homosexual male interacting, the lady didn’t feel confident to put her real name, the one connected with mainstream horror popularity, on any of her erotica, at least initially. She also came under a good amount of criticism from the feminist community at the time, especially for the “Beauty” books, seeing as the main character in these books was a sub-female.
‘Outing’ herself with Belinda (and all too soon revealing herself also as A.N. Roquelaure), Rice let the world know that she was a prolific writer of all kinds of fiction and proud to be so. In fact, the plot of Belinda, which I will only reveal enough of to make my point here, sees the main character confronted with the fact that he is coming to create art that is changing his life, is the most important stuff he has ever made, but will, if revealed, certainly jeopardize the art he is known for and has gained his popularity from.
Yes, art imitates life and vice versa.
I loved me some Anne Rice from here on in… as if I didn’t love the lady already! I even met her around this time and had a quick yet spirited exchange with her at a book signing, where she called me “darling.” And seeing as I was undergoing my own little mini-artistic consideration at the time, beginning to write erotica for the first time, while penning children’s songs and writing mainstream sci-fi, I could relate to the story of Belinda and what it seemed to mean to Anne Rice.
So, now with this wonderful writer, fantastically friendly lady, and spectacular erotica writer dead, I felt I needed to take a column here and pay tribute, in my small way, to one of the best writers of our age, Anne Rice.







 FS: What first inspired you to get into the pleasure products industry?
FS: What first inspired you to get into the pleasure products industry? 3
3













 You can tell a lot about someone’s personality from the sex position they like best. If classic Missionary is your go-to, then you may be romantic, but not very adventurous, or if Sideways is your favorite, you may be the cuddly, cozy type. But whatever your preference, the New Year gives you a reason to expand your repertoire, try something new and think outside the sex box!
You can tell a lot about someone’s personality from the sex position they like best. If classic Missionary is your go-to, then you may be romantic, but not very adventurous, or if Sideways is your favorite, you may be the cuddly, cozy type. But whatever your preference, the New Year gives you a reason to expand your repertoire, try something new and think outside the sex box!